Volume 15, Number 2—February 2009
Dispatch
Genomic Characterization of Novel Human Parechovirus Type
Abstract
Using a simple metagenomic approach, we identified a divergent human parechovirus (HPeV) in the stool of a child in Pakistan. Genomic characterization showed this virus was distinct enough from reported HPeV types to qualify as candidate prototype for the seventh HPeV type.
Human parechoviruses (HPeVs) belong to the recently identified genus Parechovirus of the family Picornaviridae. Serologic and molecular studies show that HPeV comprises 6 neutralization serotypes or corresponding types based on capsid protein similarities, HPeV1–6. HPeV1 and HPeV2, originally known as enterovirus echoviruses 22 and 23, were isolated in 1956 (1). Because echoviruses 22 and 23 had serologic, molecular, and biologic properties highly distinct from other enteroviruses, they were reclassified in 1999 as members of the genus Parechovirus (2). The other 4 parechovirus types were identified more recently from young children with clinical manifestations similar to those caused by human enteroviruses: HPeV3 in 2002 (3), HPeV4 in 2005 (4), and HPeV5 (5) and HPeV6 (6) in 2006. HPeV infections occur commonly in the general population and mostly cause mild gastrointestinal and respiratory symptoms in young children (7). More severe consequences also have been ascribed to HPeV infections, including acute flaccid paralysis (AFP) (3), encephalitis (8), aseptic meningitis (9), myocarditis (10), neonatal sepsis (11), and Reye syndrome (6),
Nonpolio AFP may be caused by many viruses, including nonpolio enteroviruses, human adenoviruses, herpes simplex, Epstein-Barr virus, and West Nile virus (12). HPeV1 was associated with an AFP outbreak in Jamaica in 1986. In 2 of 3 AFP patients with HPeV1 detected in stool samples, antibody titer also increased significantly (13). HPeV6 was isolated from the stool specimen of an AFP patient in Japan in 2001 (6). HPeV3 has not been reported from AFP cases but was identified in 1 transient paralysis case and believed to cause serious central nervous system symptoms more frequently than HPeV1 (3,7). HPeV types 2, 4, and 5 have been less often observed in clinical studies.
Using sequence-independent PCR amplification and sequence similarity searches, we recently investigated virus sequences in stool samples from children in Pakistan who had nonpolio AFP and from healthy children who had close contacts with persons who had AFP. Sequences of human parechoviruses were identified in samples from 6 of 65 persons. Analysis showed 5 HPeV infections in 56 samples from persons who had nonpolio AFP, 1 HPeV1, 1 HPeV5, and 2 HPeV6; in 1 sample, HPeV type could not be determined because the sequenced fragment was located in a phylogenetically uninformative region. A highly divergent HPeV type also was identified in 1 contact sample, and the full genome of this virus was sequenced. Phylogenetic analysis indicated that this virus, designated PAK5045, has the genetic characteristics expected of a new HPeV type.
HPeV PAK5045 was found in 1 stool sample from a healthy 2-year-old boy who had close contact with a person who had nonpolio AFP, using a previously described method applied here to stool samples (14). Briefly, virus nucleic acids were purified from stool samples, randomly amplified by reverse transcription (RT)–PCR using 3′ randomized RT and PCR primers, subcloned, and sequenced. HPeV sequences were abundant in 1 sample with 24/48 plasmid subclones identified as PAK5045. Assembly of these HPeV sequences produced 5 fragments covering ≈75% of the genome. Specific PCR primers were used to link these genome fragments, and rapid amplification of cDNA ends was carried out to acquire the 5′ and 3′ ends.
The nucleotide sequence of PAK5045 virus was 7,127 nt, excluding a poly (A) tail. PAK5045 contained a partial 5′ untranslated region (UTR) of 511 nt, an open reading frame (ORF) encoding a putative polyprotein precursor of 2,175 aa, and a 3′ UTR of 88 nt. The nucleotide sequence of PAK5045 was generated with at least 2× coverage except for the 5′ UTR. The full-length sequence of PAK5045 has been deposited in GenBank under accession no. EU556224.
The polyprotein of PAK5045 comprised capsid proteins VP0 (289 aa), VP3 (254 aa), and VP1 (226 aa) and nonstructural proteins 2A (149 aa), 2B (122 aa), 2C (329 aa), 3A (117 aa), 3B (20 aa), 3C (200 aa), and 3D (469 aa). Comparison of the complete ORF of PAK5045 with the 6 HPeV prototypes showed it was closely related to HPeVs and had amino acid identity of 84.8%–89.1% and nucleotide identity of 75.6%–80.8% (Table 1). Of the 6 known HPeV types, the intertype amino acid identities ranged from 84.9% to 91.1%, and the intertype nucleotide identities of the ORF sequence ranged from 76.1% to 83.4% (data not shown), a range similar to their identities relative to PAK5045.
Figure 1

Figure 1. Phylogenetic analysis of PAK5045 virus (arrows) and parechovirus strains based on A) the complete amino acid sequence of P1 region and B) the complete amino acid sequence of viral protein 1...
Phylogenetic analysis with the complete P1 amino acid sequences of fully sequenced HPeVs confirmed the existence of the 6 types defined by previous studies (Figure 1, panel A) (15). PAK5045 virus was most similar to HPeV3 strains. The identity of P1 amino acid sequences between PAK5045 virus and both HPeV3 strains analyzed was 77.5%, which was lower than some HPeVs intertype amino acid identities (e.g., average of 82.4% between HPeV1 and HPeV2, 78.3% between HPeV1 and HPeV4, 80.4% between HPeV1 and HPeV6, 78.4% between HPeV2 and HPeV6, and 80.5% between HPeV4 and HPeV5) (data not shown).
Consistent with the P1 amino acid tree, phylogenetic analysis with VP1 capsid proteins also showed 6 established types (Figure 1, panel B) (5). PAK5045 VP1 was slightly closer to type 3 strains, with the greatest amino acid identity being 78.8% (Table 2), and more divergent from the other established HPeV types. We retrieved from GenBank, and then analyzed, genetic relationships among 92 full-length VP1 amino acid sequences and with PAK5045. None clustered with PAK5045 as a close genetic lineage. The amino acid identities between PAK5045 and HPeV3 strains ranged from 69.9% to 78.8%, outside the HPeV3 intratype range of 85.8%–100% (Table 2).
The PAK5045 polyprotein contained 9 putative cleavage sites at VP0/VP3 (T/A), VP3/VP1 (Q/N), VP1/2A (E/S), 2A/2B (Q/G), 2B/2C (Q/G), 2C/3A (Q/T), 3A/3B (E/R), 3B/3C(Q/R), and 3C/3D (Q/G). Alignments showed that VP3/VP1, VP1/2A, and 2C/3A cleavage sites differed for PAK5045 relative to those of fully sequenced HPeVs strains, whereas the other 6 sites were conserved. The cleavage site in VP0/VP3 of PAK5045 was identical to that of HPeV2 but not to those of other types. The VP1/2A cleavage site was identical between PAK5045 and HPeV3 strains A308/99 and Can82853-01 but not other HPeVs. The RGD motif (arginine-glycine-aspartic acid) at the C terminus of VP1 was absent in PAK5045 and in HPeV3 strains A308/99 and Can82853-01, which indicates that mechanisms other than RGD binding to integrins may occur during PAK5045 infection.
Figure 2
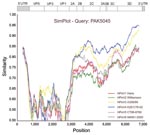
Figure 2. SimPlot (http://sray.med.som.jhmi.edu/SCRoftware/simplot) analysis of the full-length sequences of the human parechovirus (HPeV) prototypes against PAK5045 query, based on nucleotide similarities. Each curve compares the PAK5045 genome with an HPeV prototype....
To identify recombination events between the different HPeV types, we performed SimPlot analysis (http://sray.med.som.jhmi.edu/SCRoftware/simplot) of the 6 complete nucleotide HPeV prototype genomes against PAK5045 (Figure 2). In general, PAK5045 was closer to HPeV3 and HPeV4 than to the other viruses. PAK5045 showed a relatively higher degree of nucleotide similarity to HPeV3 A308/99 in the P1 region consistent with the P1 phylogenetic tree. Downstream of nucleotide position 3600, HPeV4 K251176-02 became the closest relative of PAK5045 in most of the nonstructural (P2/3) region, which suggests an ancient recombination event.
We identified and characterized a novel HPeV type from the stool sample of a healthy children who had been in close contact with person who had nonpolio AFP. The genome sequence diverged sufficiently from the 6 known HPeVs to qualify as a candidate for the prototype of HPeV7. Using only a low-level shotgun sequencing method, we detected HPeVs in 9% (6/65) of stool samples from patients with nonpolio AFP, including HPeV types 1, 5, 6, and 7. A more sensitive method, such as HPeV-directed RT-nested PCR, is likely to have detected a higher prevalence. The median age of sampled patients was 3 years (range 1 month–15 years), and all HPeV-positive patients were <3 years of age.
In a previous study, HPeVs were isolated from 0.3% of 13,656 various clinical samples collected in Japan (14 HPeV1, 16 HPeV3, 10 HPeV6, and 1 HPeV4) (6). In Germany, the detection rate of HPeVs did not differ significantly between patients with acute diarrhea and controls, with 11.6% (7/60) of children <2 years of age being HPeV positive (15). In a Dutch study of 303 isolates showing cytopathic effects consistent with enterovirus infection, 12% were HPeV positive, with 27 HPeV1 and 10 HPeV3, all in children <3 years of age (7). HPeV infection, therefore, seems to be associated with young children (<3 years). More studies are needed to associate HPeV infection (with any genotypes) with development of neurologic disease, such as AFP.
Dr Li is a research fellow at the Blood Systems Research Institute, San Francisco. Her current research interest focuses on discovery of novel viruses using metagenomic methods.
Acknowledgments
We thank Flavien Bernardin and Elisabeth Slikas for helpful suggestions in phylogenic analyses.
This work was supported by National Institutes of Health grant R01 HL083254 to E.D.
References
- Wigand R, Sabin AB. Properties of ECHO types 22, 23 and 24 viruses. Arch Gesamte Virusforsch. 1961;11:224–47. DOIPubMedGoogle Scholar
- King AMQ, Brown F, Christian P, Hovi T, Hyypia T, Knowles NJ, Picornaviridae. In: Van Regenmortel MHV, Fauquet CM, Bishop DHL, Calisher CH, Carsten EB, Estes MK, et al. (editors). Virus taxonomy: the seventh report of the International Committee on Taxonomy of Viruses. New York: Academic Press; 1999.
- Ito M, Yamashita T, Tsuzuki H, Takeda N, Sakae K. Isolation and identification of a novel human parechovirus. J Gen Virol. 2004;85:391–8. DOIPubMedGoogle Scholar
- Benschop KS, Schinkel J, Luken ME, van den Broek PJ, Beersma MF, Menelik N, Fourth human parechovirus serotype. Emerg Infect Dis. 2006;12:1572–5.PubMedGoogle Scholar
- Al-Sunaidi M, Williams CH, Hughes PJ, Schnurr DP, Stanway G. Analysis of a new human parechovirus allows the definition of parechovirus types and the identification of RNA structural domains. J Virol. 2007;81:1013–21. DOIPubMedGoogle Scholar
- Watanabe K, Oie M, Higuchi M, Nishikawa M, Fujii M. Isolation and characterization of novel human parechovirus from clinical samples. Emerg Infect Dis. 2007;13:889–95.PubMedGoogle Scholar
- Benschop KS, Schinkel J, Minnaar RP, Pajkrt D, Spanjerberg L, Kraakman HC, Human parechovirus infections in Dutch children and the association between serotype and disease severity. Clin Infect Dis. 2006;42:204–10. DOIPubMedGoogle Scholar
- Legay V, Chomel JJ, Fernandez E, Lina B, Aymard M, Khalfan S. Encephalomyelitis due to human parechovirus type 1. J Clin Virol. 2002;25:193–5. DOIPubMedGoogle Scholar
- Stanway G, Joki-Korpela P, Hyypia T. Human parechoviruses—biology and clinical significance. Rev Med Virol. 2000;10:57–69. DOIPubMedGoogle Scholar
- Russell S, Bell E. Echoviruses and carditis. Lancet. 1970;1:2.
- Boivin G, Abed Y, Boucher FD. Human parechovirus 3 and neonatal infections. Emerg Infect Dis. 2005;11:103–5.PubMedGoogle Scholar
- Kincaid O, Lipton HL. Viral myelitis: an update. Curr Neurol Neurosci Rep. 2006;6:469–74. DOIPubMedGoogle Scholar
- Figueroa JP, Ashley D, King D, Hull B. An outbreak of acute flaccid paralysis in Jamaica associated with echovirus type 22. J Med Virol. 1989;29:315–9. DOIPubMedGoogle Scholar
- Kapoor A, Victoria J, Simmonds P, Wang C, Shafer RW, Nims R, A highly divergent picornavirus in a marine mammal. J Virol. 2008;82:311–20. DOIPubMedGoogle Scholar
- Baumgarte S, de Souza Luna LK, Grywna K, Panning M, Drexler JF, Karsten C, Prevalence, types, and RNA concentrations of human parechoviruses, including a sixth parechovirus type, in stool samples from patients with acute enteritis. J Clin Microbiol. 2008;46:242–8. DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleTable of Contents – Volume 15, Number 2—February 2009
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Eric Delwart, Blood Systems Research Institute, 270 Masonic Ave, San Francisco, CA 94118, USA
Top