Volume 23, Number 7—July 2017
Research
Novel Retinal Lesion in Ebola Survivors, Sierra Leone, 2016
Paul J. Steptoe , Janet T. Scott, Julia M. Baxter, Craig K. Parkes, Rahul Dwivedi, Gabriela Czanner, Matthew J. Vandy, Fayiah Momorie, Alimamy D. Fornah, Patrick Komba, Jade Richards, Foday Sahr, Nicholas A.V. Beare, and Malcolm G. Semple
, Janet T. Scott, Julia M. Baxter, Craig K. Parkes, Rahul Dwivedi, Gabriela Czanner, Matthew J. Vandy, Fayiah Momorie, Alimamy D. Fornah, Patrick Komba, Jade Richards, Foday Sahr, Nicholas A.V. Beare, and Malcolm G. Semple
Figure 2
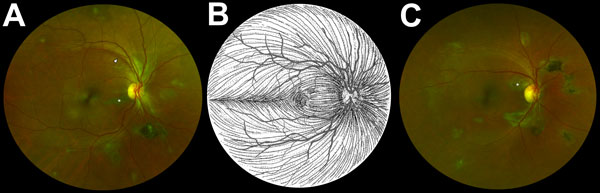
Figure 2. Composite scanning laser ophthalmoscope retinal images showing type 6 Ebola peripapillary and peripheral lesions, observed following the anatomic distribution of the ganglion cell axons (retinal nerve fiber layer), in a case–control study of ocular signs in Ebola virus disease survivors, Sierra Leone, 2016. A) Example 1, right eye. B) Illustration of the ganglion cell axon anatomic distribution. Courtesy of W.L.M. Alward. C) Example 2, right eye. Asterisks indicate curvilinear lesions distinct from the retinal vasculature. White arrowhead indicates retinal nerve fiber wedge defect.
Page created: June 19, 2017
Page updated: June 19, 2017
Page reviewed: June 19, 2017
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.