Volume 29, Number 3—March 2023
Dispatch
Correlation of High Seawater Temperature with Vibrio and Shewanella Infections, Denmark, 2010–2018
Abstract
During 2010–2018 in Denmark, 638 patients had Vibrio infections diagnosed and 521 patients had Shewanella infections diagnosed. Most cases occurred in years with high seawater temperatures. The substantial increase in those infections, with some causing septicemia, calls for clinical awareness and mandatory notification policies.
Vibrio and Shewanella spp. bacteria cause a variety of human infections, including wound infections, ear infections, septicemia, and gastroenteritis (1). Domestically acquired Vibrio and Shewanella infections occur only sporadically in countries in northern Europe because the coastal seawater temperature tends to be too cold to support growth and high bacterial pathogen concentration levels (2,3). However, the warming of low-salinity coastal waters of the Baltic Sea has promoted the growth of Vibrio and Shewanella spp. and consequently increased the risk of disease for humans exposed to such seawater (4). In the unusually warm summer of 1994 in Denmark, several V. vulnificus and S. algae infections were seen among patients who reported bathing in seawater (5,6). Furthermore, during 2014–2018, more than 1,055 cases of vibriosis were reported in northern Europe countries, including Denmark (7).
Considering the annual increase in infections during recent summer seasons in Denmark and the recurring heatwaves across Europe, this emerging public health threat requires more investigation to provide decision-makers with evidence for action. The aim of our nationwide study was to describe the distribution of Vibrio and Shewanella infections in Denmark during 2010–2018 and investigate a possible correlation between infections and sea surface temperature.
We studied cases of Vibrio and Shewanella infections during 2010–2018 in the summer months in Denmark (June to August); in the decade spanning 2010–2020, 2018 was the warmest registered summer in the country. We obtained information about the cases from the Danish Microbiology Database, a national database containing all clinical microbiology reports from Denmark (8). We extracted identification results, confirmed by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry, on Vibrio and Shewanella spp. cultured from blood, wound swabs, deep soft tissue, ear, trachea, urine, and feces as well as information about date of sampling. We also extracted the person identification number of each patient studied from Denmark’s Central Person Registry (CPR) (9). Clinical patient information was not available, but sample types were used as a proxy for type of infection. We registered cases by month per patient (Appendix 1). We counted the number of cases by calendar year and stratified them by the genus of isolated bacterial pathogen. Using the CPR number, we eliminated duplicate positive results. By linking to data from the CPR register, we retrieved information on address of residence for each case at the time of sampling. We performed geomapping and geocoding in QGIS 1.8.0 Lisboa (https://www.qgis.org) for the spatial analysis of Shewanella and Vibrio cases and plotting of number of infections per municipality, which we further interpreted based on seawater salinity in the mapped areas. We obtained sea surface temperatures of the coastal waters of Denmark during summer from the Danish Meteorological Institute (Appendix 1; Appendix 2). We performed the Pearson correlation test in R version 4.2.1 (The R Foundation for Statistical Computing, https://www.r-project.org) to determine correlation between annual summer seawater temperatures and number of Vibrio and Shewanella cases.
Figure 1

Figure 1. Relationship between Shewanella and Vibrio spp. infections and seawater temperature in Denmark, by year, 2010–2018. A, B) Pearson correlation between annual numbers of diagnosed ...
We found a positive correlation between average summer seawater temperatures (15°C–22°C) and the number of cases of Vibrio (29–172) and Shewanella (18–134) infections diagnosed in Denmark during 2010–2018 (p<0.0001; Figure 1, panels A, B). Results showed a higher number of infections during warmer summers compared with colder summers. Ear infections (n = 595) and wound infections (n = 424) were the most frequent clinical manifestations (Table); V. alginolyticus and S. algae were predominant in ear infections. V. parahaemolyticus was the most frequently isolated from wounds (n = 103, 24%), V. vulnificus (n = 14, 36%) and S. putrefaciens (n = 10, 26%) were predominant in septicemia cases, and S. putrefaciens was the species most associated with deep soft tissue infections (Table). Clinical manifestations varied by bacterial species. More than one third of V. vulnificus infections manifested as septicemia, supporting evidence of the high virulence of this species (10–12).
Vibrio and Shewanella infections increased during every summer in the study period. The summers of 2014 and 2018 were characterized by particularly high sea surface temperatures and showed an association to higher incidence in infections (Figure 1, panels A, B). In all studied years, the frequency of Vibrio and Shewanella spp. infections increased beginning in week 23, reaching a peak in the warmest months (July and August), followed by a tail of decreasing number in subsequent months (Appendix 1 Figure, panel A). A recent study on 2018 data alone reported that most human vibriosis cases reported in the Nordic region were likely linked to exposure to the warm seawater that year (7). We found that infections were more prevalent in men and boys 10–19 years of age and in elderly persons, 60–80 years of age (Appendix 1 Figure, panel B). We suspect that those results are likely because active adolescents may have scratches or wounds while performing recreational water activities (e.g., swimming, rowing, windsurfing, or fishing) and because of the vulnerability of elderly persons in general.
Figure 2
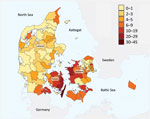
Figure 2. Number of cases of Shewanella and Vibrio spp. infection (n = 98), by municipality, Denmark, 2018.
We found a marked geographic distribution in results obtained from 2018, when most cases were in persons who lived near coastal areas with brackish waters characterized by low saline levels (<30 parts per thousand; Figure 2) (13). In contrast, along the west coast of Jutland, where the salinity of the North Sea is high and the water colder, the frequency of infections was lower. This difference suggests that increased temperature of low-salinity water favors the growth of Vibrio and Shewanella bacteria. It is important to consider that the association between place of residence and number of cases is challenged because geographic distances are short in Denmark and multiple exposures at different geographic sites during a summer season are to be expected. The lack of information on prior seawater exposure and information on international travel for each case is a limitation for the correlation between number of Vibrio and Shewanella infections and seawater exposure. Nevertheless, the observed geographic distribution of cases and the presented correlation between the number of cases in cold and warm summers strongly supports a relationship between higher-temperature/low-saline seawater exposure and risk of infection.
In this nationwide study, we show a correlation between number of Vibrio and Shewanella human infections and coastal summer water temperature in Denmark during 2010–2018. In addition, we were able to map residency of most cases to geographic areas with coastlines of low salinity. A combination of climate change effects (i.e., increasing coastal sea surface temperature at higher latitudes during summer) and a more elderly population indicates the need for increased awareness of the risk of these emerging infections and their public health impact. Rising temperatures will lead to an increase in burden of disease for these marine infections in an expanding area of the northern hemisphere (14). We propose that persons in Denmark who are exposed to seawater in summer should consider covering open wounds with a waterproof bandage, particularly the elderly and immunocompromised. We also recommend that persons thoroughly wash new cuts exposed to seawater and inform healthcare professionals of recent seawater exposure when seeking medical attention. Persons with defected eardrums should use earplugs. Our study lends support to categorizing all Vibrio and Shewanella infections in humans as mandatory notifiable diseases in Denmark and other countries in Europe that have seawater borders to monitor the incidence of these infections.
Dr. Hounmanou is a postdoctoral fellow at the University of Copenhagen. He conducts research in microbial genomics on human pathogens that arise from animals and the aquatic environment and addresses questions related to climate change implications on disease transmission between humans and waterbodies, such as cholera and other Vibrio infections.
Acknowledgments
The authors thank the Danish Microbiology Database board of representatives and the departments of clinical microbiology in Denmark. We also extend our gratitude to Naja Stolberg Bahrenscheer for assistance with drawing the map.
This study was conducted based on administrative register data. According to Denmark law, ethics approval is not needed for such research. The study is covered by the legal acts regulating national surveillance of infectious diseases.
References
- Tantillo GM, Fontanarosa M, Di Pinto A, Musti M. Updated perspectives on emerging vibrios associated with human infections. Lett Appl Microbiol. 2004;39:117–26. DOIPubMedGoogle Scholar
- Baker-Austin C, Trinanes JA, Taylor NGH, Hartnell R, Siitonen A, Martinez-Urtaza J. Emerging Vibrio risk at high latitudes in response to ocean warming. Nat Clim Chang. 2013;3:73–7. DOIGoogle Scholar
- Gram L, Bundvad A, Melchiorsen J, Johansen C, Fonnesbech Vogel B. Occurrence of Shewanella algae in Danish coastal water and effects of water temperature and culture conditions on its survival. Appl Environ Microbiol. 1999;65:3896–900. DOIPubMedGoogle Scholar
- Baker-Austin C, Trinanes JA, Salmenlinna S, Löfdahl M, Siitonen A, Taylor NGH, et al. Heat wave-associated vibriosis, Sweden and Finland, 2014. Emerg Infect Dis. 2016;22:1216–20. DOIPubMedGoogle Scholar
- Dalsgaard A, Frimodt-Møller N, Bruun B, Høi L, Larsen JL. Clinical manifestations and molecular epidemiology of Vibrio vulnificus infections in Denmark. Eur J Clin Microbiol Infect Dis. 1996;15:227–32. DOIPubMedGoogle Scholar
- Holt HM, Søgaard P, Gahrn-Hansen B. Ear infections with Shewanella alga: a bacteriologic, clinical and epidemiologic study of 67 cases. Clin Microbiol Infect. 1997;3:329–34. DOIPubMedGoogle Scholar
- Amato E, Riess M, Thomas-Lopez D, Linkevicius M, Pitkänen T, Wołkowicz T, et al. Epidemiological and microbiological investigation of a large increase in vibriosis, northern Europe, 2018. Euro Surveill. 2022;27:
2101088 . DOIPubMedGoogle Scholar - Voldstedlund M, Haarh M, Mølbak K; MiBa Board of Representatives. The Danish Microbiology Database (MiBa) 2010 to 2013. Euro Surveill. 2014;19:20667. DOIPubMedGoogle Scholar
- Schmidt M, Pedersen L, Sørensen HT. The Danish civil registration system as a tool in epidemiology. Eur J Epidemiol. 2014;29:541–9. DOIPubMedGoogle Scholar
- Frank C, Littman M, Alpers K, Hallauer J. Vibrio vulnificus wound infections after contact with the Baltic Sea, Germany. Euro Surveill. 2006;11:
E060817.1 .PubMedGoogle Scholar - Li G, Wang MY. The role of Vibrio vulnificus virulence factors and regulators in its infection-induced sepsis. Folia Microbiol (Praha). 2020;65:265–74. DOIPubMedGoogle Scholar
- Horseman MA, Surani S. A comprehensive review of Vibrio vulnificus: an important cause of severe sepsis and skin and soft-tissue infection. Int J Infect Dis. 2011;15:e157–66. DOIPubMedGoogle Scholar
- Kniebusch M, Meier HEM, Radtke H. Changing salinity gradients in the Baltic Sea as a consequence of altered freshwater budgets. Geophys Res Lett. 2019;46:9739–47. DOIGoogle Scholar
- Trinanes J, Martinez-Urtaza J. Future scenarios of risk of Vibrio infections in a warming planet: a global mapping study. Lancet Planet Health. 2021;5:e426–35. DOIPubMedGoogle Scholar
Figures
Table
Cite This ArticleOriginal Publication Date: February 15, 2023
Table of Contents – Volume 29, Number 3—March 2023
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Yaovi Mahuton Gildas Hounmanou, Department of Veterinary and Animal Sciences, University of Copenhagen, Stigbøjlen 4, 1870 Frederiksberg, Denmark;gil@sund.ku.dk
Top