Volume 29, Number 4—April 2023
Dispatch
Emergence and Persistent Dominance of SARS-CoV-2 Omicron BA.2.3.7 Variant, Taiwan
Abstract
Since April 2022, waves of SARS-CoV-2 Omicron variant cases have surfaced in Taiwan and spread throughout the island. Using high-throughput sequencing of the SARS-CoV-2 genome, we analyzed 2,405 PCR-positive swab samples from 2,339 persons and identified the Omicron BA.2.3.7 variant as a major lineage within recent community outbreaks in Taiwan.
The COVID-19 pandemic, caused by SARS-CoV-2, originated in China in late 2019, probably in the city of Wuhan (1,2). The outbreak of this unusual respiratory disease led to a wide variety of responses by various countries across the world (3–6). The response in Taiwan was rapid and based on both its proximity to China and its experiences during the SARS pandemic ≈2 decades earlier (5,7,8). The introduction of strict travel restrictions on incoming air and sea passengers, long compulsory quarantine periods for the few residents allowed to enter Taiwan, and a vast public acceptance of safety measures (e.g., social distancing, temperature checks, mask wearing) resulted in a delay in the emergence of the COVID-19 pandemic in Taiwan compared with other countries (5,9,10). Until April 2022, there were only limited outbreaks, all of which were quickly contained. Taiwan therefore provides a unique opportunity to explore what happened when the Omicron variant finally evaded the controls put in place by the Taiwan government and began to spread through the country’s population.
Residents of Taiwan had not been exposed, on a large scale, to any of the virus variants before Omicron. By the time SARS-CoV-2 began to spread widely in Taiwan April 2022, there had been around 17,000 recorded cases of COVID-19 in the country, and most of them were linked to the Alpha variant (almost all cases in our study had not been infected with SARS-CoV-2 before). Vaccination rates of Taiwan’s population at that time were 82.7% having received 1 dose, 78% having received 2 doses, and 59.1% having received 3 doses. The vaccines used in Taiwan before May 2022 were the Oxford-AstraZeneca vaccine (https://www.astrazeneca.com), the Pfizer-BioNTech vaccine (https://www.pfizer.com), the Moderna vaccine (https://www.modernatx.com), the Johnson & Johnson/Janssen vaccine (https://www.jandj.com), and The Median vaccine (a protein subunit COVID-19 vaccine made in Taiwan). Most residents of Taiwan received doses of the first 3 vaccines.
Figure 1
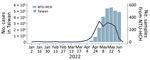
Figure 1. Weekly statistics for confirmed COVID-19 cases in Taiwan and sequenced samples, lineage distribution, and mutation prevalence derived from the NTU-HCH surveillance program, January–June 2022. Graph shows the number of COVID-19...
Very few COVID-19 cases occurred in Taiwan during 2020 and 2021. Clustered infections were reported in May and June 2021, mainly in northern Taiwan. Even at the peak, only hundreds of positive cases were recorded by Taiwan’s Centers for Disease Control. Early in 2022, several Omicron infection clusters were noted, first in northern Taiwan, and new cases quickly followed, soon exceeding 50,000 per day, with outbreaks affecting the entire country (Figure 1) (Infectious Disease Statistics Query System, https://nidss.cdc.gov.tw/nndss/disease?id=19CoV).
Figure 2

Figure 2. Phylogenetic analysis of SARS-CoV-2 sequences based on 1,966 sequences from the NTU-HCH surveillance program in Taiwan and 881 sequences from GISAID (https://www.gisaid.org). Lineages of NTU-HCH strains are annotated...
To gain insights into community transmission and to monitor viral evolution, we deployed a genomic surveillance protocol at National Taiwan University Hospital Hsinchu Branch (NTU-HCH) whereby we performed whole-genome sequencing on nasal swab samples detected by PCR to be positive for SARS-CoV-2 (Appendix 1). To ensure data quality, we submitted genomic data to GISAID (https://www.gisaid.org) only on those sequences that had >98% coverage of the 29,903-bp SARS-CoV-2 target genome. We used the same set of high-quality sequences for tracking the signature mutations in the viral samples (Table 1) and for phylogenetic analysis (Figure 2; Appendix 1, Figure 1). We found 2,405 samples among 5 batches that met the above criterion and this generated 2,043 sequences (84.9% pass rate). We selected 1,966 sequences for GISAID submission (Appendix 1 Table 1).
We analyzed the assembled viral genome sequences (Appendix 1 Table 2) and tracked the lineages and nonsynonymous amino acid changes in the Omicron samples collected during 2022 (Appendix 1 Figures 2, 3). Comparing the later 3 datasets (batches 3–5), we discovered that 3 amino acid changes (open reading frame [ORF]1a: L631F; spike (S): K97E; nucleocapsid; M322I) occurred only after the fourth sequencing batch. The percentage of sequences containing the signatures progressed steadily from 62% in batch 4 to 85% in batch 5. All batch-3 isolates belonged to the BA.1 or BA.2 classification, suggesting that the rapid increase of cases in Taiwan in April and May 2022—from 0 cases/day to ≈100,000 cases/day—came from a strain (BA.2.3.7) that might have been involved in a founder effect.
To construct the framework of the phylogenetic tree, we took 1,966 genome sequences from our study and analyzed them in the global context of 881 GISAID reference sequences (Figure 2; Appendix 2). We then zoomed in and compared the 1,577 Omicron sequences of our study against the 228 Omicron BA.2.3.7 strains from GISAID. Those sequences were reported from 21 countries, including 51 from Taiwan (Table 2). We conducted phylogenetic analysis using the Pango-dynamic nomenclature system (11).
We found evidence that this novel lineage BA.2.3.7 with 3 amino acid changes (ORF1a: L631F; S: K97E; and nucleocapsid: M322I) was circulating dominantly in Taiwan over the study period. Of note, the first BA.2.3.7 strain identified in the epidemic in Taiwan was collected on March 27, 2022, and since that time we detected several genomic changes affecting this Omicron lineage. For example, we noted a new mutation, G1251V (Appendix 1 Figure 3, green line) in the S protein, from April onward, and that particular circulating lineage then rapidly spread across Taiwan.
We acknowledge that our study is limited in that we conducted the genomic surveillance in only 1 medical center; therefore, the observed dominance of BA.2.3.7 might be due to clustering of cases. Of note, while this paper was in preparation, we became aware that several viral sequences with the same signature mutations had been reported in Taiwan. Although the number of cases was relatively small (51) compared with the number of cases we studied, the 4 locations in Taiwan reporting those cases were different from our collection point at the hospital. Thus, this new lineage appeared to be broadly detectable across Taiwan.
Other Asia-Pacific countries have also recently reported a substantial cumulative prevalence of the BA.2.3.7 variant (Table 2). Among the 44 Omicron BA.2.3.7 strains reported from Japan, 2 of the affected persons had travel history to Vietnam and 41 to Taiwan, suggesting considerable silent outward transmission from Taiwan. In contrast, BA.2.3.7 accounts for <0.5% of the sequences reported in either California, USA, or globally. The emergence of Omicron BA.2.3.7 in Asia is remarkable. Because there are no reliable genomic data from early cases in Malaysia and Vietnam, our phylogenic analysis and the metadata from GISAID suggests that travel between countries in Asia contributed to the rapid spread of this unique Omicron lineage.
In summary, our genomic dataset is uniquely valuable for understanding how a major COVID-19 outbreak occurs in a naive and vaccinated population in Taiwan, a country with a very limited number of entry events. We theorize that the dominant circulation of BA.2.3.7 in Taiwan is likely the result of genetic drift or a founder effect, although it is also possible that increased transmissibility or vaccine evasion played some part. As countries in Asia move from zero tolerance to more open COVID-19 policies, continued surveillance of SARS-CoV-2 using next-generation sequencing is important. Early detection of viral evolution events in endemic areas will help minimize future disruptions caused by a new variant.
Dr. Shao is an assistant professor in the Department of Laboratory Medicine and Pediatrics, National Taiwan University College of Medicine, Taiwan. Her main research interests include infectious disease, clinical virology, clinical microbiology, and vaccines. Dr. Tu is postdoctoral fellow in the Institute of Molecular and Genomic Medicine, National Health Research Institutes, Taiwan. Her research interests include next generation sequencing technology, cancer, and genomic research. Dr. Gong is an assistant professor in Research Center for Emerging Viral Infections and International Master’s Degree Program for Molecular Medicine in Emerging Viral Infections, Chang Gung University, Taiwan. His research interests include bioinformatics, phylogenetics, machine learning, and viral evolution.
Acknowledgments
We extend our thanks to Y. Henry Sun and Hsiao-Hui Tso for critical reading of the manuscript; Yi-Chun Tsai, Shuo-Peng Chou, Jhen-Rong Huang, and Yuan-Yu You for sample collection and nucleic acid preparation; and Tai-Yun Lin, Yu-Chen Huang, and Chiao-Chan Wang for library construction and sequencing operation. We gratefully acknowledge the authors from the originating laboratories responsible for obtaining the specimens as well as the submitting laboratories where the genome data were generated and shared via GISAID and GenBank (Appendix 2).
This work was supported by Ministry of Health and Welfare of Taiwan (MOHW110-TDU-C-222-000010) to S.F.T., by the Research Center for Emerging Viral Infections from The Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education of Taiwan, the Ministry of Science and Technology of Taiwan (MOST 111-2321-B-182-001, MOST 111-2634-F-182-001, MOST 110-2222-E-182-004, and MOST 111-2221-E-182-053-MY3), and the National Institute Of Allergy And Infectious Diseases of the National Institutes of Health under Award Number 5U01AI151698-02 to Y.N.G. and S.R.S.
References
- World Health Organization. WHO statement regarding cluster of pneumonia cases in Wuhan, China. January 9, 2020 [cited 2023 Jan 26]. https://www.who.int/china/news/detail/09-01-2020-who-statement-regarding-cluster-of-pneumonia-cases-in-wuhan-china
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al.; China Novel Coronavirus Investigating and Research Team. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382:727–33. DOIPubMedGoogle Scholar
- Mathieu E, Ritchie H, Rodés-Guirao L, Appel C, Giattino C, Hasell J, et al. Coronavirus pandemic (COVID-19). Our world in data [cited 2023 Jan 26]. https://ourworldindata.org/coronavirus
- Jung AS, Haldane V, Neill R, Wu S, Jamieson M, Verma M, et al. National responses to covid-19: drivers, complexities, and uncertainties in the first year of the pandemic. BMJ. 2021;375:
e068954 . DOIPubMedGoogle Scholar - Summers J, Cheng HY, Lin HH, Barnard LT, Kvalsvig A, Wilson N, et al. Potential lessons from the Taiwan and New Zealand health responses to the COVID-19 pandemic. Lancet Reg Health West Pac. 2020;4:
100044 . DOIPubMedGoogle Scholar - Tsou HH, Kuo SC, Lin YH, Hsiung CA, Chiou HY, Chen WJ, et al. A comprehensive evaluation of COVID-19 policies and outcomes in 50 countries and territories. Sci Rep. 2022;12:8802. DOIPubMedGoogle Scholar
- Chen SC. Taiwan’s experience in fighting COVID-19. Nat Immunol. 2021;22:393–4. DOIPubMedGoogle Scholar
- Wang CJ, Ng CY, Brook RH. Response to COVID-19 in Taiwan: Big data analytics, new technology, and proactive testing. JAMA. 2020;323:1341–2. DOIPubMedGoogle Scholar
- Gong YN, Tsao KC, Hsiao MJ, Huang CG, Huang PN, Huang PW, et al. SARS-CoV-2 genomic surveillance in Taiwan revealed novel ORF8-deletion mutant and clade possibly associated with infections in Middle East. Emerg Microbes Infect. 2020;9:1457–66. DOIPubMedGoogle Scholar
- Lin C, Braund WE, Auerbach J, Chou JH, Teng JH, Tu P, et al. Policy decisions and use of information technology to fight coronavirus disease, Taiwan. Emerg Infect Dis. 2020;26:1506–12. DOIPubMedGoogle Scholar
- Rambaut A, Holmes EC, O’Toole Á, Hill V, McCrone JT, Ruis C, et al. A dynamic nomenclature proposal for SARS-CoV-2 lineages to assist genomic epidemiology. Nat Microbiol. 2020;5:1403–7. DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleOriginal Publication Date: March 14, 2023
1These authors contributed equally to this article.
Table of Contents – Volume 29, Number 4—April 2023
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Chong-Jen Yu, NTUH, Hsin-Chu Branch, Sec. 1 Shengyi Rd, Zhubei, Hsinchu 30261, Taiwan
Top