Volume 17, Number 9—September 2011
Research
Increasing Incidence of Invasive Haemophilus influenzae Disease in Adults, Utah, USA
Abstract
Since the introduction of the Haemophilus influenzae type b vaccine, the incidence of invasive H. influenzae type b disease among children has fallen dramatically, but the effect on invasive H. influenzae disease among adults may be more complex. In this population-based study we examined the epidemiology and outcomes of invasive disease caused by typeable and nontypeable H. influenzae among Utah adults during 1998–2008. The overall incidence increased over the study period from 0.14/100,000 person-years in 1998 to 1.61/100,000 person-years in 2008. The average incidence in persons >65 years old was 2.74/100,000 person-years, accounting for 51% of cases and 67% of deaths. The incidence was highest for nontypeable H. influenzae (0.23/100,000 person-years), followed by H. influenzae type f (0.14/100,000 person-years). The case-fatality rate was 22%. The incidence of invasive H. influenzae in Utah adults appears to be increasing. Invasive H. influenzae infection disproportionately affected the elderly and was associated with a high mortality rate.
Before the introduction of the Haemophilus influenzae type b (Hib) conjugate vaccine, Hib was the most common cause of bacterial meningitis in children <5 years of age (1,2). Hib caused >80% of invasive H. influenzae disease among children (3). Since the introduction of the Hib conjugate vaccine, the incidence of invasive Hib disease in children has decreased by 99% (1,2). Several studies have reported a decrease in the incidence of invasive Hib in adults following widespread use of vaccine in children (4,5).
However, although the decrease in the overall incidence of invasive disease caused by Hib for children and adults has been a remarkable public health success, changes in the epidemiology of invasive disease caused by other H. influenzae have been observed. The incidence of H. influenzae invasive disease has shifted toward adults. In a study conducted in the Atlanta, Georgia, USA, metropolitan area before Hib vaccine introduction, adults comprised 24% of all invasive H. influenzae cases (6). A more recent population-based report from Illinois showed adults accounting for 77% of invasive cases (7). Other encapsulated strains, including H. influenzae type a (Hia), have emerged as notable causes of invasive disease among children in Utah, Alaska, and the Navajo nation (8–10). Given the changing epidemiology observed elsewhere, we sought to describe the epidemiology of invasive H. influenzae infections among Utah adults during 1998 through 2008.
Study Design and Population
We identified all cases of laboratory-confirmed invasive H. influenzae among Utah residents >18 years of age reported to the Utah Department of Health (UDoH) from 1998 through 2008. Invasive H. influenzae is an immediately reportable condition in Utah. We defined invasive H. influenzae according to the Council of State and Territorial Epidemiologists definition: a clinically compatible case that is confirmed by isolation of H. influenzae from a normally sterile site such as blood, cerebrospinal fluid, joint fluid, pleural fluid, or pericardial fluid (11). The UDoH enhanced their passive surveillance program in 2005 by sending out reminders to major laboratories in Utah to report invasive H. influenzae cases. As part of these enhancement efforts, 1 large laboratory also began automated case reporting to the UDoH in 2005. Because these changes in surveillance could introduce ascertainment bias for the final 4 years of this analysis, we conducted a parallel retrospective cohort analysis of laboratory-confirmed invasive H. influenzae cases among Utah residents within the Intermountain Healthcare (IH) system during 1999–2008 (on the basis of availability of complete laboratory data). IH is a vertically integrated hospital system that provides care to roughly 50% of Utah adults (Scott Lloyd, pers. comm.). The estimated market share by age group is recalculated at regular intervals. Over this period, IH made no major changes to its microbiology practices that would alter the recovery of H. influenza isolates.
Serotyping
H. influenzae isolated from sterile sites was identified by using standard culture techniques. Laboratories are requested to submit sterile site isolates of H. influenzae to the Utah Public Health Laboratory in Salt Lake City, Utah, for definitive serotyping by using monovalent antisera for H. influenzae types a–f. Isolates from reported H. influenzae cases not sent to the Utah Public Health Laboratory for serotyping were classified as not typed. All other isolates were classified as Hia–f or as nontypeable.
Demographic and Outcome Data
As part of its surveillance program, the UDoH collected demographic information including county of residence, race/ethnicity, age, gender, hospitalization, and death. Starting in 2005, the UDoH began to collect expanded clinical information including the presence of chronic medical conditions and clinical signs. These clinical data were collected at the local health department level. It should be noted that not all local health departments conducted such data collection, and collection methods varied across local health departments (e.g., chart review, patient interview, hospital information personnel interview).
Statistical Analysis
To calculate the incidence rate, we used the estimated annual Utah population among persons >18 years of age on the basis of the United States 2000 census (12). To derive an incidence for the IH cohort, we multiplied the estimated annual population by IH estimated market share of adult healthcare in Utah for a given year. Market share data were only available for 2000, 2002, and 2005–2008. For intervening years, we extrapolated using available data for the nearest years.
Categorical variables were evaluated by using standard χ2 test for independence or Fisher exact test as appropriate. To evaluate associations between variables, we used ordinary logistic regression and exact logistic regression as appropriate. Poisson regression method with a log-linear model was performed to test for trend variation in the annual case rates for the IHC and UDoH datasets. We used SAS version 9.2 (SAS Institute Inc., Cary, NC, USA) for all statistical analyses.
Human Subjects Protection
We obtained approval for this study from the Institutional Review Boards of the University of Utah and IH; de-identified case information was provided by the UDoH through a data sharing agreement. Informed consent was waived as all data were de-identified.
Figure 1

Figure 1. Comparison of annual incidence of invasive Haemophilus influenzae disease derived from the Utah Department of Health and Intermountain Healthcare databases, Utah, USA, 1998–2008. Black line, Intermountain Healthcare; red line, Utah Department...
We identified 121 cases of invasive H. influenzae in Utah adults reported to the UDoH during 1998–2008 (Table). The incidence of H. influenzae invasive disease was 0.66 cases per 100,000 person-years averaged over the 11 years. Incidence increased over the study period from 0.14 cases per 100,000 person-years in 1998 to a peak in 2008 of 1.61 cases per 100,000 person-years (p = 0.0023, by linear test for trend) (Figure 1). We observed a marked seasonality with winter predominance: 41.3% of cases occurring in winter, 26.4% in spring, 21.4% in fall, and 10.7% in summer. We observed no significant difference in distribution between sexes, with 64 cases in women and 57 cases in men (p = 0.65).
The incidence rates estimated by using the IH data showed a similar trend (Figure 1). We identified 94 cases of invasive H. influenzae, with an estimated average annual incidence of 1.05/100,000 person-years. The incidence increased from 0.54/100,000 person-years in 1999 to 1.27/100,000 person-years in 2008 (p = 0.002, by linear test for trend). Although the estimated rates differed, the trend in increasing incidence was similar for both data sources.
Figure 2
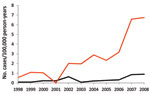
Figure 2. Annual incidence of invasive Haemophilus influenzae disease in adults, by age, Utah, USA, 1998–2008. Red line, age >65 y; black line, ages 18–64 y.
The incidence of invasive disease was markedly higher among persons >65 years of age; the average incidence in this age group was 2.74 cases per 100,000 person-years and increased to 6.14 cases per 100,000 in 2008. The average incidence for persons 18–34, 35–49, and 50–64 years of age were 0.25, 0.26, and 0.88 per 100,000 person-years, respectively. Compared with persons 18–34 years of age, patients >65 years of age had a 12-fold greater risk for invasive disease (risk ratio 12.5, 95% confidence interval [CI] 7.29–21.32; p<0.0001). The incidence of invasive disease increased significantly over the study period among those >65 years of age (Figure 2).
Serotype Distribution
Figure 3
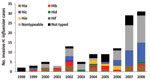
Figure 3. No. cases of invasive Haemophilus influenzae (Hi) disease in adults, by serotype (a–f), Utah, USA, 1998–2008.
Of the 121 patients with invasive disease, 101 (83%) isolates were serotyped. Figure 3 depicts the annual number of cases by serotype and isolates that did not undergo serotype testing. Nontypeable strains accounted for 43 cases (43%). Hib accounted for 9 cases (9%) and non-b encapsulated strains accounted for 49 cases (49%). Serotypes f and a accounted for 25 (25%) and 15 cases (15%), respectively.
The increases in invasive disease were largely because of nontypeable strains and Hif. The average incidence over 11 years of invasive disease caused by nontypeable strains was 0.23/ 100,000 person-years, and rose from 0 in 1998 and 1999 to an average of 0.72/100,000 person-years during 2007 and 2008. During 1998–2008, the average incidence of disease caused by Hif was 0.14/100,000 person-years and rose to an average of 0.48/100,000 person-years during 2007 and 2008. The number of cases of Hia remained relatively steady, with an average annual incidence of 0.08/100,000 person-years.
Clinical Disease
Most (51%) invasive disease occurred in persons >65 years of age. Bacteremia accounted for 83% of all cases, meningitis for 12.4%, and other sterile sites for the remaining 4.6%. Nontypeable strains, Hib, and Hif accounted for 13 of the 15 cases of meningitis (Table). Infection with Hib was significantly more likely to be associated with meningitis than nontypeable strains (odds ratio [OR] 6.1, 95% CI 1.3–29.0). While invasive disease was more likely to occur in the elderly, a greater proportion of disease among patients 18–49 years of age was due to meningitis compared with patients >50 years of age (25% vs. 9%; p = 0.05).
Data on underlying illness was available for 69 of the 121 case-patients. Forty-six (67%) of 69 patients had chronic medical conditions; 33% had >2. Twenty-four patients had diabetes mellitus; 15 were immunocompromised; 14 had chronic lung disease; 11 had a malignancy; 3 had asthma; 3 each had chronic obstructive pulmonary disease, congestive heart failure, chronic liver disease/cirrhosis, and chronic kidney disease; and 1 had a history of intravenous drug use. Forty-six patients had a diagnosis of pneumonia at the time of H. influenzae isolation. Patients with pneumonia were significantly more likely to have >1 chronic illness (OR 4.48, 95% CI 1.48–13.58, p = 0.008) and significantly less likely to have meningitis (OR 0.048, 95% CI 0–0.358, p = 0.0016).
The overall case-fatality rate was 22%. Two thirds of deaths were among those >65 years of age. Persons >65 years of age had a case-fatality rate of 29% compared to 15% for those <65 years of age (p = 0.08). The case-fatality rate for patients with bacteremia (23%) was not significantly higher than for patients with meningitis (13%). The case-fatality rate did not differ significantly by serotype. Outcome did not differ significantly by the presence or absence of concurrent conditions (17% vs. 26% mortality rate, respectively), but data were only available for 69 patients.
Despite the virtual elimination of Hib in areas with widespread use of Hib vaccine, invasive disease caused by H. influenzae remains a major source of illness and death. The incidence of invasive H. influenzae in Utah adults appears to be increasing; most of the increase in H. influenzae disease incidence was attributable to an increase in nontypeable and Hif strains. We found that invasive H. influenzae disease was most common in persons >65 years of age and was associated with a high mortality rate.
The overall incidence of invasive H. influenzae disease in adults in our population, 0.66 cases per 100,000 person-years, was similar to rates observed in Illinois (1.0/100,000 person-years in 1994) (7) and slightly lower than rates among Alaskans during 1991–1996 (1.4/100,000 person-years) (5). We found a significant increase in the incidence of invasive H. influenzae over the study period by using 2 surveillance methods. Several studies in addition to ours suggest an increase in invasive disease caused by to non-type b H. influenzae among adults (5,7,13). The reasons for this change are unclear, and might reflect changes in the organisms, changes in the number of persons at high risk, or perhaps waning of cross-immunity induced by exposure to Hib.
As the prevalence of Hib has decreased, other encapsulated serotypes seem to have emerged as major causes of invasive disease, including Hif in Illinois and Hia in Brazil, Manitoba, and Northwestern Ontario (7,10,14,15). Similar to findings in Illinois, Hif was the second most common serotype in our analysis (25%), and cases of invasive Hif contributed substantially to the increase of invasive H. influenzae cases we observed in 2007–2008. Although Hia was the third most common isolate among adults in our study, it accounted for only 15% of all cases, a rate that is much lower than rates in Manitoba (29%) (15), Northwestern Ontario (42%) (10), and in children in Utah (8).
Nontypeable H. influenzae has been the most common isolate in virtually all published series among adults. In our study, it accounted for 43% of cases; similar rates were reported in other studies (3,7,15–17). The emerging role of invasive disease because of nontypeable strains is intriguing because this organism has traditionally been considered a relatively noninvasive bacteria predominantly associated with community-acquired pneumonia, chronic obstructive pulmonary disease exacerbations, and otitis media (18). Whether invasive strains of nontypeable H. influenzae have distinct genotypic and phenotypic characteristics compared with noninvasive isolates remains largely unknown. Candidate virulence factors include the adhesin genes hmw and hia and IS1016, an insertion element that may confer Hib-like, encapsulated properties to nontypeable strains. However, to date no single set of virulence determinants has been conclusively associated with invasive nontypeable strains (19–21). Better understanding of the factors that confer invasive capabilities might lead to improved strategies for vaccine development.
Similar to the findings in Spain, Illinois, and Alaska, rates of disease in our study were highest among older patients (3,5,7). The incidence increased in persons >65 years of age, and 29% of infections in this age group were fatal, emphasizing the disproportionate effect. Invasive H. influenzae was highly associated with concurrent illness. Among those for whom clinical data were available, 67% of our patients had an underlying condition, as has been observed in other studies (3,7). However, in those with and without concurrent illness, invasive H. influenzae showed a high overall case-fatality rate (22%). Other studies have reported that invasive H. influenzae is associated with high mortality rates, ranging from 13% to 29% (3,4,6,7). During 2005–2008, the CDC Active Bacterial Core surveillance reported case-fatality rates of 13%–17% for invasive H. influenzae (22). Among adults >65 years of age, the incidence of invasive H. influenzae, the case-fatality rate and the number of attributable deaths exceeds that for invasive meningococcal disease in the most vulnerable age group, those 11–19 years of age (23). However, no vaccine is available for invasive disease caused by encapsulated non-type b and nontypeable H. influenzae. Efforts to prevent invasive H. influenzae, particularly among the elderly, should become a public health priority.
As with all surveillance studies, our study is subject to several limitations. The UDoH relies on passive reporting of H. influenzae from laboratories throughout the state, making underreporting likely. However, a study of invasive H. influenzae in Spain among children <5 years of age demonstrated that passive surveillance had a sensitivity of 88% (24). Comparison of estimated rates from the IH laboratory database and UDoH surveillance data suggests that the sensitivity of reporting among adults was 65%. Changes in reporting behavior and changes to the passive surveillance program in 2005 are potential sources of bias. Several studies have demonstrated the inaccuracy of serotyping compared with molecular diagnostic techniques (25,26). Although serotyping is still an accepted standard, had we performed capsular gene analysis, it might have changed the serotype distribution. Additionally, the small number of identified cases places limitations on analyses of serotype distribution and clinical characteristics. Finally, we had clinical information on concurrent conditions for only 57% of the cohort, and clinical information was not collected in a systematic manner across the state.
These limitations notwithstanding, we found that the incidence of invasive H. influenzae in Utah adults appears to be increasing, and this increase is caused mostly by the rising incidence of nontypeable H. influenzae and Hif. Invasive H. influenzae, including disease caused by nontypeable strains, has a high mortality rate. Persons >65 years of age are most affected by the disease and have the highest death rates. These data have implications for targeted adult H. influenzae vaccine development.
Dr Rubach just completed an Internal Medicine–Pediatrics combined residency at the University of Utah and began a fellowship in infectious diseases within the Department of Internal Medicine at Duke University in July 2011. His research interests include molecular diagnostics with field applications in nonindustrialized countries.
Acknowledgments
We thank IH and all Utah hospital microbiology laboratories for their continued efforts in H. influenzae reporting, and Melissa Stevens-Dimond for her support in data collection.
A.T.P. is supported by grants from the National Institute of Allergy and Infectious Diseases (U01AI082184-01) and the Centers for Disease Control and Prevention (U18-IP000303-01).
References
- Centers for Disease Control and Prevention. Progress toward eliminating Haemophilus influenzae type b disease among infants and children–United States, 1987–1997. MMWR Morb Mortal Wkly Rep. 1998;47:993–8.PubMedGoogle Scholar
- Bisgard KM, Kao A, Leake J, Strebel PM, Perkins BA, Wharton M. Haemophilus influenzae invasive disease in the United States, 1994–1995: near disappearance of a child vaccine preventable disease. Emerg Infect Dis. 1998;4:229–37. DOIPubMedGoogle Scholar
- Campos J, Hernando M, Roman F, Perez-Vazquez M, Aracil B, Oteo J, Analysis of invasive Haemophilus influenzae infections after extensive vaccination against H. influenzae type B. J Clin Microbiol. 2004;42:524–9. DOIPubMedGoogle Scholar
- Sarangi J, Cartwright K, Stuart J, Brookes S, Morris R, Slack M. Invasive Haemophilus influenzae in adults. Epidemiol Infect. 2000;124:441–7. DOIPubMedGoogle Scholar
- Perdue DG, Bulkow LR, Gellin BG, Davidson M, Petersen KM, Singleton RJ, Invasive Haemophilus influenzae disease in Alaskan residents aged 10 years and older before and after infant vaccination programs. JAMA. 2000;283:3089–94. DOIPubMedGoogle Scholar
- Farley MM, Stephens DS, Brachman PS, Harvey RC, Smith JD, Wenger JD, Invasive Haemophilus influenzae disease in adults. Ann Intern Med. 1992;116:806–12.PubMedGoogle Scholar
- Dworkin MS, Park L, Borchardt SM. The changing epidemiology of invasive Haemophilus influenzae disease, especially in persons >65 years old. Clin Infect Dis. 2007;44:810–6. DOIPubMedGoogle Scholar
- Bender JM, Cox CM, Mottice S, She RC, Korgenski K, Daly JA, Invasive Haemophilus influenzae disease in Utah children: an 11-year population-based study in the era of conjugate vaccine. Clin Infect Dis. 2010;50:e41–6. DOIPubMedGoogle Scholar
- Millar EV, O’Brien KL, Watt JP, Lingappa J, Pallipamu R, Rosenstein N, Epidemiology of invasive Haemophilus influenzae type a disease among Navajo and White Mountain Apache children, 1988–2003. Clin Infect Dis. 2005;40:823–30. DOIPubMedGoogle Scholar
- Brown VM, Madden S, Kelly L, Jamieson FB, Tsang RS, Ulanova M. Invasive Haemophilus influenzae disease caused by non–type b strains in northwestern Ontario, Canada, 2002–2008. Clin Infect Dis. 2009;49:1240–3. DOIPubMedGoogle Scholar
- Centers for Disease Control and Prevention. Case definitions for infectious conditions under public health surveillance. MMWR Recomm Rep. 1997;46:1–55.PubMedGoogle Scholar
- Utah population over 18 years old. Utah’s Indicator-Based Information System for Public Health [cited 2009 Apr15]. http://ibis.health.utah.gov/querty/selection/pop/PopSelection.html
- Ladhani S, Slack MPE, Heath PT, von Gottberg A, Chandra M, Ramsay ME, Invasive Haemophilus influenzae disease, Europe, 1996–2006. Emerg Infect Dis. 2010;16:455–63. DOIPubMedGoogle Scholar
- Ribeiro GS, Reis JN, Cordeiro SM, Lima JBT, Gouveia EL, Petersen M, Prevention of Haemophilus influenzae type b (Hib) meningitis and emergence of serotype replacement with Type A strains after introduction of Hib immunization in Brazil. J Infect Dis. 2003;187:109–16. DOIPubMedGoogle Scholar
- Tsang RS, Sill ML, Skinner SJ, Law DKS, Zhou J, Wylie J. Characterization of invasive Haemophilus influenzae disease in Manitoba, Canada, 2000–2006: invasive disease due to non–type b strains. Clin Infect Dis. 2007;44:1611–4. DOIPubMedGoogle Scholar
- Bajanca P, Canica M; Multicenter Study Group. Emergence of nonencapsulated and encapsulated non–b-type invasive Haemophilus influenzae isolates in Portugal. J Clin Microbiol. 2004;42:807–10. DOIPubMedGoogle Scholar
- Ladhani S, Ramsay ME, Chandra M, Slack MP. EU-IBIS. No evidence for Haemophilus influenzae serotype replacement in Europe after introduction of the Hib conjugate vaccine. Lancet Infect Dis. 2008;8:275–6. DOIPubMedGoogle Scholar
- Murphy TF. Haemophilus infections. In: Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson L, et al., editors. Harrison’s Internal Medicine. 17th ed. New York: McGraw-Hill; 2008. p. 923–6.
- Erwin AL, Nelson KL, Mhlanga-Mutangadura T, Bonthuis PJ, Geelhood JL, Morlin G, Characterization of genetic and phenotypic diversity of invasive nontypeable Haemophilus influenzae. Infect Immun. 2005;73:5853–63. DOIPubMedGoogle Scholar
- St Geme JW, Takala A, Esko E, Falko S. Evidence for capsule gene sequences among pharyngeal isolates of nontypeable Haemophilus influenzae. J Infect Dis. 1994;169:337–42. DOIPubMedGoogle Scholar
- Satola SW, Napier B, Farley MM. Association of IS1016 with the hia adhesin gene and biotypes V and I in invasive nontypeable Haemophilus influenzae. Infect Immun. 2008;76:5221–7. DOIPubMedGoogle Scholar
- Centers for Disease Control and Prevention Active Bacterial Core Surveillance Reports [cited 2009 Oct 25]. http://www.cdc.gov/abcs/survreports.htm
- Bilukha OO, Rosenstein N; National Center for Infectious Diseases. Prevention and control of meningococcal disease. MMWR Recomm Rep. 2005;54:1–21.PubMedGoogle Scholar
- Domínguez A, Bou R, Carmona G, Latorre C, Pineda V, Sanchez F, Working Group on Invasive Disease Caused by Haemophilus influenzae. Invasive disease caused by Haemophilus influenzae: the sensitivity of statutory reporting. Ann Epidemiol. 2004;14:31–5.PubMedGoogle Scholar
- Bokermann S, Zanella RC, Lemos AP, de Andrade AL, Brandileone MC. Evaluation of methodology for serotyping invasive and nasopharyngeal isolates of Haemophilus influenzae in the ongoing surveillance in Brazil. J Clin Microbiol. 2003;41:5546–50. DOIPubMedGoogle Scholar
- Satola SW, Collins JT, Napier R, Farley MM. Capsule gene analysis of invasive Haemophilus influenzae: accuracy of serotyping and prevalence of IS1016 among nontypeable isolates. J Clin Microbiol. 2007;45:3230–8. DOIPubMedGoogle Scholar
Figures
Table
Cite This ArticleTable of Contents – Volume 17, Number 9—September 2011
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Matthew P. Rubach, Division of Infectious Diseases, Box 102359, Duke University Medical Center, Rm 156, Hanes House, Trent Dr, Durham, NC 27710, USA
Top